The Asian Indian Phenotype: Why Your BMI Is Normal but Your Belly Fat Is Dangerous
Indians develop metabolic disease at far lower body weights than the global BMI chart suggests. Here's the biology behind it.
ALTRcare Medical Team
Clinical Editorial
You're not "that overweight." The scale is fine, your BMI reads normal or just borderline — and yet your last report flagged high triglycerides, a fatty liver, or pre-diabetes. If you're Indian, that contradiction isn't bad luck. It's biology, and it has a name.
BMI was built for European bodies
The familiar cut-offs — overweight at 25, obese at 30 — came from studies of European populations. Indians develop metabolic disease at far lower body weights, which is why Indian guidelines quietly lowered the thresholds years ago: overweight begins at a BMI of 23, obesity at 25. By the standard global chart, millions of metabolically sick Indians look perfectly healthy.
The "thin-fat" body
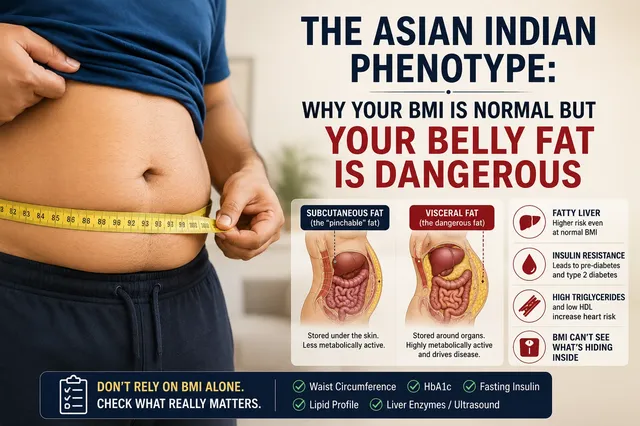
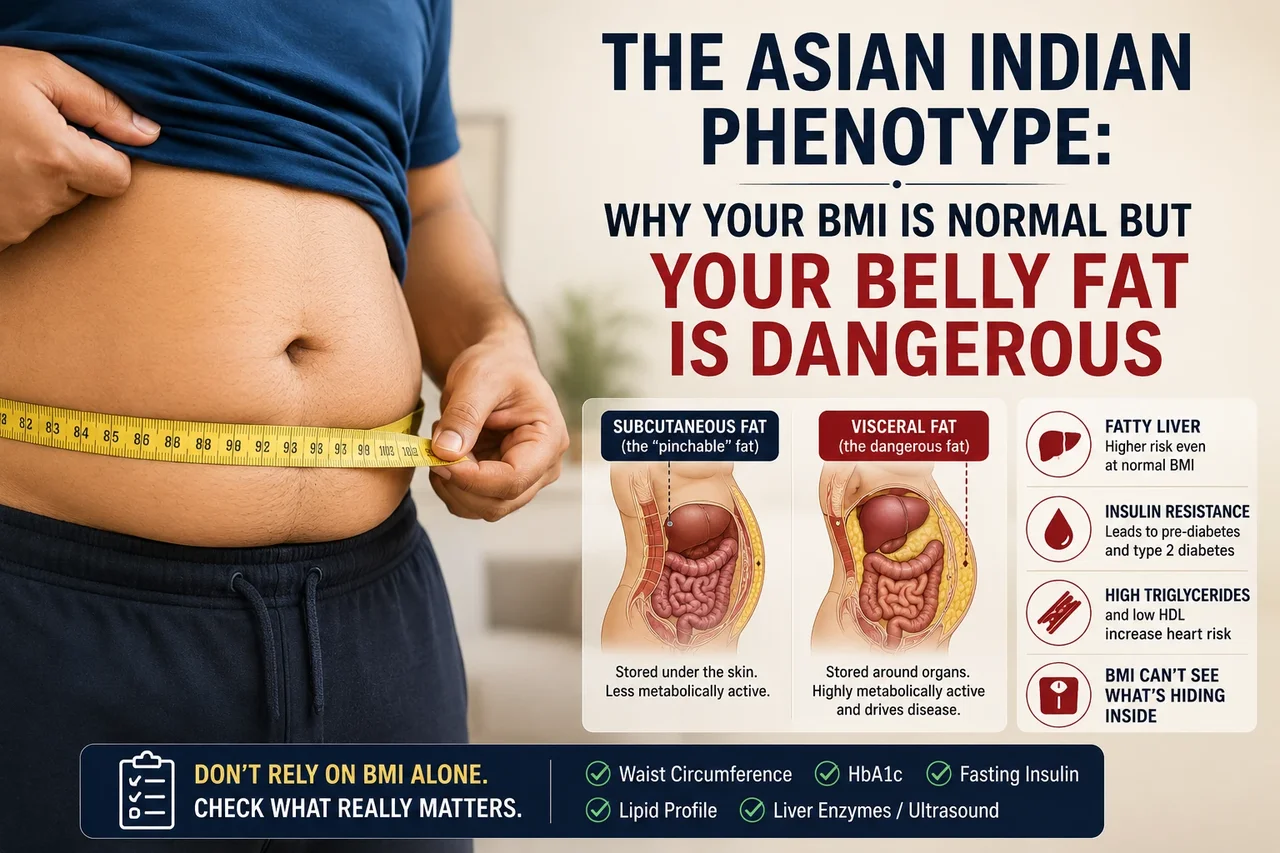
At the same weight, Asian Indians tend to carry less muscle and more fat than Europeans. More importantly, that fat parks itself in the worst possible place — wrapped around the liver, pancreas and intestines as visceral fat — rather than under the skin. The result is the classic skinny-fat silhouette: slim arms, slim legs, a soft central belly. The mirror lies to you.
Why visceral fat is the dangerous kind
Subcutaneous fat, the kind you can pinch, is relatively harmless. Visceral fat is metabolically active. It pumps inflammatory signals and free fatty acids straight into the liver, driving insulin resistance, fatty liver, high triglycerides and low HDL. This is the engine behind why India has become one of the diabetes capitals of the world while many patients never looked "fat" at all.
Why diet and the gym often don't fix it
You cannot spot-reduce visceral fat with crunches, and once insulin resistance has set in, a plain calorie deficit becomes an uphill fight against your own hormones. That's a trap worth understanding on its own — see [why you're not losing weight in a calorie deficit](/blog/insulin-resistance-trap).
Where GLP-1 medicines fit
Doctor-supervised GLP-1 therapy (semaglutide, tirzepatide) does two things that matter here: it improves insulin sensitivity, and it shifts the body toward burning the visceral fat that diet alone struggles to reach — while quieting the appetite signals that keep the cycle going.
What to actually do
Stop trusting BMI alone. Ask for the numbers that see visceral fat: waist circumference (Indian risk starts above 90 cm for men and 80 cm for women), fasting insulin or HbA1c, a lipid panel, and a liver ultrasound or enzymes. If those are off despite a "normal" weight, you're not imagining it.
An ALTRcare doctor can read your full metabolic picture and tell you whether medication is even appropriate for you. If cost is what's stopping you, read [why the molecule is now cheap but the supervision isn't](/blog/ozempic-cost-india).
Frequently asked questions
Is BMI useless for Indians?
Not useless, but misleading on its own. Indians develop metabolic disease at lower BMIs, so a "normal" BMI can hide significant visceral fat. Pair it with waist circumference and blood markers.
What waist size is considered risky for Indians?
Indian guidelines flag raised risk above roughly 90 cm for men and 80 cm for women — lower thresholds than the older Western numbers.
Can I have a normal weight and still need treatment?
Yes. If you have high visceral fat with insulin resistance, fatty liver, or an adverse lipid profile, you may benefit from treatment even at a normal BMI. A doctor should assess this individually.
Ready to take the next step?
Take the free 2-minute eligibility assessment. A doctor reviews it before anything is prescribed — no obligation.
This article is for general educational purposes and is not a substitute for personalised medical advice. GLP-1 medications are prescription-only and not suitable for everyone. Always consult a qualified doctor before starting, changing, or stopping any treatment.